B3Care Background
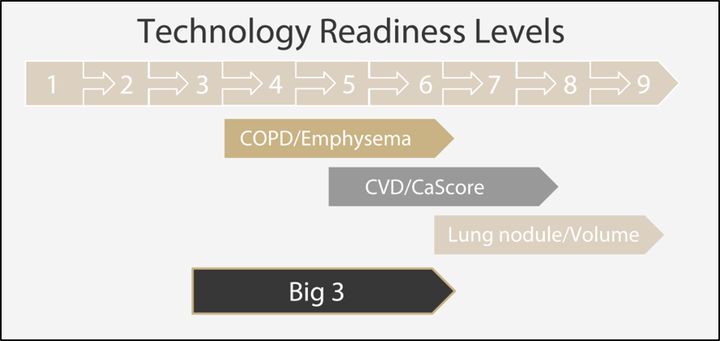 Technology Readiness Level
Technology Readiness Level
Abstract
Lung cancer, chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD), the so-called Big-3 (B3), are expected to cause most deaths by 2050. Early detection and prevention are crucial to lower the disease burden. Innovative low-dose computed tomography (CT) allows simultaneous, integrated assessment of early imaging biomarkers of lung cancer, COPD and CVD. Major advantages of integrated B3 screening are expected due to shared risk factors, B3 interdependence and health economic yield comparison to single disease screening. However, a major impediment before establishing a B3 screening program is the lack of validated and standardized B3 imaging biomarkers. The aim of this project is to advance the technology readiness level (TRL) of integrated B3 screening with at least 2 levels. To reach this objective, B3CARE will develop a large, high-quality imaging data biobank to provide biomarker reference values and validate B3 biomarkers using novel image analysis software and novel machine learning approaches. This will accelerate software development for CT-imaging data post-processing. Also, the expected substantial health economics potential of combined B3 imaging biomarkers for personalized health strategies is evaluated. B3CARE will thus provide an invaluable resource for the accelerated development and implementation of B3 imaging biomarkers and computer aided decision support.
Background
Lung cancer, chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD) are highly prevalent in the general Dutch population (annual incidences: Lung cancer n=12,200, COPD n=53,300, and CVD n=101,700) resulting in a high burden on the health system and associated healthcare costs, annually in total 10 billion euros [National Institute of Public Health and Environment 2015 (in Dutch)]. For this so-called Big3 (or B3), early detection and treatment will cure many patients in time and delay or stop disease progression. Therefore, prevention and early detection are crucial. Currently, no screening is performed for the Big-3. The impact of low-dose computed tomography (CT) lung cancer screening on lung cancer stage shift and reduction of lung cancer mortality has been demonstrated [van Klaveren 2009; Aberle 2011]. In addition to the evaluation of imaging biomarkers of early lung cancer, the same CT image data set can be used to detect early signs of CVD and COPD. This part of the data has not been explored yet. Combined screening for the B3 using ultra-low-dose CT provides the next-generation technological strategy and has a highly cost-effective potential.
Ultimate ambition & challenges ahead
The ultimate ambition is to establish an integrated B3 CT screening program to enable effective personalized prevention and early treatment strategies aimed at reducing B3 morbidity and mortality. CT lung cancer screening has proven survival benefit in long-term smokers [Aberle 2011]. It is likely that it will be implemented in Europe within the next 5 years [Oudkerk 2017]. Additional benefit of integral CT screening for CVD and COPD requires further exploration. Major advantages of integrated B3 screening can be anticipated due to shared risk factors and thus overlapping at-risk population, simultaneous presence of B3 diseases, and the health economic yield compared to a single disease. The latest advances in innovative ultra-low-dose CT, for the first time, enable the early simultaneous assessment of imaging biomarkers of lung cancer, COPD and CVD, and enable the potential for integral B3 screening. However, there are several impediments that are to be addressed in the preparation and establishment of a B3 screening program. Challenges include the lack of validated and standardized B3 imaging biomarkers, particularly for COPD. Another hurdle is the labour-intensive work required to obtain B3 imaging biomarkers. Also, education and training for evaluation of B3 CT screening examinations is lacking. Finally, the cost-efficiency of integral B3 screening has not been established.
An imaging biomarker is a decision parameter to assess disease presence, absence, activity, or outcome in individuals or groups with the disease process [Buckler 2011]. Validation and standardization of these measurements is essential to ensure that quantitative measurements are accurate and precise. Researchers from CMINEN and MDII have been heavily involved in technical and clinical validation of lung nodule volumetry as imaging biomarker for lung cancer [Heuvelmans 2013; Zhao 2013; Xie 2014; Horeweg 2014; Walter 2016], calcium scoring as imaging biomarker for CVD [Vliegenthart 2003; van Ooijen 2005; Groen 2007; Elias-Smale 2010; Vonder 2017], and bronchial wall thickness and lung density as imaging biomarkers for COPD [Mets 2011; Lo 2012; Mohamed Hoesein 2014; Petersen 2014; Pompe 2015, 2016]. This has resulted in validated measurements for lung nodule volumetry and calcium scoring. However, these validated measurements have been manually performed and are labour intensive. Further development of automated software tools and algorithms are important to make B3 screening feasible and sustainable; these can be validated against the image data biobank we will establish in this project. For COPD imaging biomarkers, further validation is needed, even more so since the first commercial products become available [Gallardo-Estrella 2016].
Additionally, to clinically validate individual imaging biomarkers, reference values of B3 imaging biomarkers within general populations need to be established, in order to be able to determine abnormal values in patients with early stages of disease. Only when an imaging feature can be accurately quantitatively measured as well as discriminate between health and (early) disease to support medical decision making, it can qualify as a biomarker. This necessitates the availability of a multi-cohort, large-scale, high-quality imaging data biobank with validated B3 imaging biomarker and outcome data, which we provide in B3CARE.

Within B3CARE, we will bring together data collections of sufficient size required for the development of novel machine learning algorithms, testing of quicker, more automated software and analysis of complex research questions. We will open the B3 imaging biobank within a research imaging data environment to researchers and post-processing developers across the world to accelerate the development and validation of B3 image biomarker software solutions, and to allow the discovery of new imaging biomarkers for B3 and other diseases. In B3CARE we will increase the TRL of B3 CT screening, the individual B3 imaging biomarkers, as well as the TRLs of the software solutions used to quantify the imaging data for use as a biomarker. The B3CARE approach provides an invaluable resource for the development and validation of B3 biomarker profiles and computer aided decision support in the context of personalized, precision and stratified medicine. Innovation will foster implementation of a B3 screening program in the Netherlands, because better algorithms are required to establish cost-effectiveness of screening.
Objective
The objective of B3CARE is to advance the technology readiness of integrated B3 screening with 2 TRLs. To reach this objective, we will develop a large, high-quality imaging data biobank and an imaging biomarker validation environment, in order to use this to technologically advance and validate biomarkers for lung cancer, COPD and CVD. This will accelerate software development for CT-imaging data post-processing. These steps are mandatory for successful implementation of integrated B3 CT screening.
Scientific background
There is increasing evidence for the benefit of low-dose CT screening to detect early lung cancer (e.g. based on our results in the NELSON trial [van Klaveren 2009, Horeweg 2013, 2014, Walter 2016] and the US NLST trial [Aberle 2011]). In case of positive mortality results in the NELSON trial (expected next year), low-dose chest CT screening will likely be implemented in the EU. Based on NELSON, lung nodule volumetry and volume doubling time have been found to be sensitive features of early lung cancer [van Klaveren 2009, Horeweg 2013, 2014, Xie 2013, 2014, Heuvelmans 2013]. Using one and the same ultra-low-dose CT scan, early imaging biomarkers of lung cancer, COPD and CVD can be assessed by one imaging modality. This is of particular importance as smoking, the main risk factor for lung cancer, is also a strong risk factor for CVD and COPD.
Coronary calcifications are quantifiable as measure of subclinical CVD. The calcium score has been extensively validated by us and others [Vliegenthart 2003, van Ooijen 2005, Groen 2007, Vonder 2017]. Previously, we have shown the strong predictive value of calcium scoring for coronary events in a population-based study [Vliegenthart 2005, Elias-Smale 2010]. At this moment, the clinical impact of CVD screening by calcium scoring, combined with evidence-based treatment, is still unknown. We are currently investigating the impact of CVD screening on morbidity and mortality in the ROBINSCA trial (sponsored by ERC-grant; radiological coordination at UMCG). Also, the reference values in a general population are lacking, for both lung nodules and calcium scoring.
Previous research in which B3CARE researchers were involved, has shown that lung density and airway wall thickness measurements can be used for early COPD detection [Mets 2011; Lo 2012; Mohamed Hoesein 2014; Petersen 2014; Pompe 2015, 2016; Sorensen 2012]. However, quantitative assessment of COPD imaging biomarkers is still under development, with different biomarkers being suggested to evaluate the extent of emphysema. Before COPD imaging biomarkers can be considered for implementation as part of the CT screening, further validation and standardization are very important, as well as correlation to clinical COPD outcomes. For this proposal, we can build on extensive experience of the research group on quantitative lung and cardiac imaging in large-scale studies, which have led to leading roles in consensus statements [Oudkerk 2008, 2017].